| |
|
积极、合理用药治疗,控制病情;辅助心灵治疗,争取实现奇迹!
|
|
| |
|
积极、合理用药治疗,控制病情;辅助心灵治疗,争取实现奇迹!
|
|
点评
谢谢憨豆兄的建议!也祝您的治疗顺利、平安!
| |
|
我是肿瘤病人,不是肿瘤医生;我的一切意见仅供参考,千万别与正规医嘱等同。
欢迎光顾:(http://blog.sina.com.cn/u/5306366644) |
|
点评
休眠疗法?突然激起我的灵感,不如试试催眠疗法?心理治疗,催眠病人,告诉他/她没有得癌症,很健康!哈哈~不知道有没有这样的尝试?
| |
|
积极、合理用药治疗,控制病情;辅助心灵治疗,争取实现奇迹!
|
|
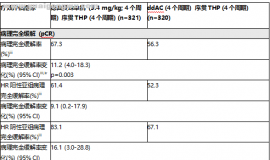
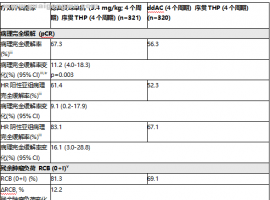 DESTINY-Breast11 III期临床研究
DESTINY-Breast11 III期临床研究:优赫得序贯THP方案术前治疗,使高风险HER2阳性早期
DESTINY-Breast11 III期临床研究
DESTINY-Breast11 III期临床研究:优赫得序贯THP方案术前治疗,使高风险HER2阳性早期
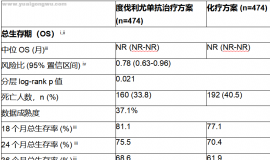
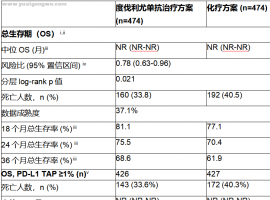 MATTERHORN III期试验中,与单独化疗
MATTERHORN III期试验中,与单独化疗相比,英飞凡治疗方案将早期胃癌患者死亡风险降低
MATTERHORN III期试验中,与单独化疗
MATTERHORN III期试验中,与单独化疗相比,英飞凡治疗方案将早期胃癌患者死亡风险降低
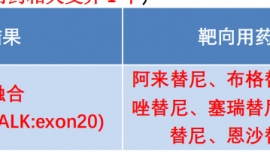
 跨越十年丨憨叔靶向轮换的感悟及思路
我们在筷子治疗九周年纪念文章《跨越九年丨憨叔靶向轮换传承和发扬 --筷子奥希替尼
跨越十年丨憨叔靶向轮换的感悟及思路
我们在筷子治疗九周年纪念文章《跨越九年丨憨叔靶向轮换传承和发扬 --筷子奥希替尼
 母亲晚期肺癌跨越13年,这是我家长期
讲述者:不怕辣椒不怕癌整理者:雪漓
在我家抗癌跨越10年之际,鹰版就曾邀请我写一篇
母亲晚期肺癌跨越13年,这是我家长期
讲述者:不怕辣椒不怕癌整理者:雪漓
在我家抗癌跨越10年之际,鹰版就曾邀请我写一篇
 它是比脑转移预后还差的转移部位,今
作者:闵
肝脏对我们的重要性不言而喻,然而治疗中不仅各种药物会对肝脏造成损伤,就
它是比脑转移预后还差的转移部位,今
作者:闵
肝脏对我们的重要性不言而喻,然而治疗中不仅各种药物会对肝脏造成损伤,就





 显身卡
显身卡 0 d a8 A' V) K+ n. j" w
0 d a8 A' V) K+ n. j" w